Outpatient Clinic
Healthcare Platform
Healthcare
Clinic Management
Eliminating System-Switching From the Clinical Workflow of a Hospital Outpatient App
Overview
A system inside hospital outpatient departments. Doctors working on it to manage their patient caseload. The engagement covered the full doctor-facing workflow: appointment scheduling and follow-up, treatment plan assignment, and procedure and operation reservation.
My Role
UX workflow designer, evaluation, interaction design, and defining the specialized components used in the final build
The Problem
Two failures were creating daily friction for every doctor using the system
Three Systems to Complete One Patient Encounter
To finish a single consultation, doctors had to leave the main system and open external tools, one to assign a treatment plan, others to reserve procedures or book operations. Every patient encounter required context-switching between systems that were never designed to work together. This broke clinical flow, added steps that served no patient purpose, and introduced decision points where errors were most likely to occur. This is the kind of fragmentation that feels like an IT problem on the surface. It isn't. It is a speed and accuracy problem. Every unnecessary switch is a moment where attention fragments and something gets missed
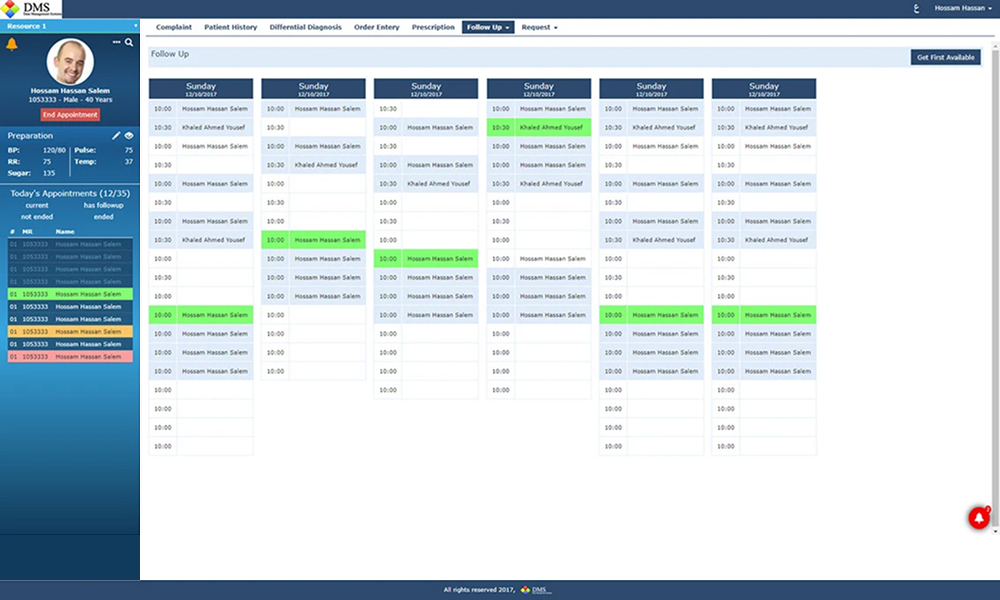
Scheduling Without Visibility
Doctors had no complete view of their appointments calendar inside the existing system. Each working session started without a clear picture of what was ahead. That missing context meant slower decisions at the very point where speed matters, when a patient is in front of you and the next steps need to be set
What I Did
Before touching any interface, the existing workflow was mapped end to end, from a doctor opening their schedule through to completing a patient encounter with a treatment plan and procedure reservation confirmed. That map made the root cause visible: the product had been built as disconnected modules, and the gaps between them had been patched with external tools rather than fixed.
Without the option of formal user research, the approach relied on direct stakeholder input and close observation of the existing workflow. The constraints were real, a tight timeline, and integration requirements across multiple external systems that had to be absorbed into a single interface without breaking the underlying connections.
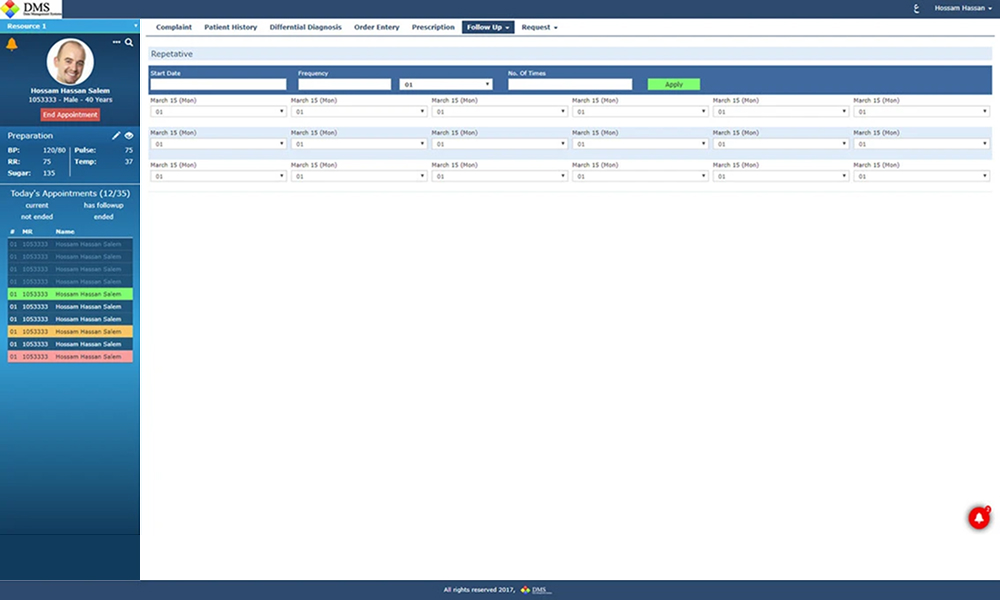
The design decision that governed everything else was consolidation. Every action a doctor needs to complete a patient encounter, follow-up scheduling, repetitive appointment reservation, treatment plan assignment, procedure reservation, had to be reachable within one flow, without leaving the interface.
The Outcome
Before
Doctors switched between multiple external systems to complete a single patient encounter
After
Every action (appointment, treatment plan, procedure reservation) handled in one interface
Following delivery, the project manager reported that the clinical flow became smoother and faster, and that doctors could make decisions quickly within a single interface. The fragmentation that had been the baseline condition was eliminated
The flow is now smoother and faster. Decisions are fast now to take by doctors
Project Manager
Hospital Outpatient System
Got a similar problem?
Let’s talk